

26 Jun Real-world evidence provided by EMA
Posted at 10:39h
in Blog
- The use of Real-World Data (RWD) is increasingly embedded in the scientific evaluation of human medicines.The newly published EMA document on the topic (Guidance on Real-world evidence provided by EMA), explains:
- how RWE, derived from analysis of RWD, can be useful in the context of regulatory decision-making,
- what types of studies can be conducted,
- how the EMA can help identify the best resources to address a research question.
An analysis of the RWD provided by the EMA could help
- to fill knowledge gaps;
- to provide independent and transparent RWE sources;
- to carry out specific analyses tailored to the individual case, e.g. to support the work of EMA’s scientific committees;
- generate evidence more quickly, shortening the process steps that an MAH would have to comply with to obtain the corresponding study approved;
- avoid unnecessary duplication and inefficiency that might be typical of studies done by industry.
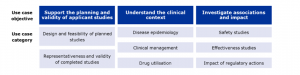
An overview of the three main areas in which RWE can support regulatory decision-making is shown in the figure below (taken from the document).
-
SOURCES:
Latest posts
-
16 December, 2024 Blog
EDQM publishes draft General Chapter “Quality of Data” for Comments








